The nurse practitioner on the other end of the phone call sounded stoic. She was calling from a rural hospital about 100 miles away from the large tertiary center ICU that I work in. She was doing her best to manage a COVID-19 patient, whose condition was declining rapidly.
“So you definitely can’t take this patient?” she asked.
“No” I said, “I’m so sorry, our ICU is full and we are no longer taking transfers” Her exasperated sigh made clear her disappointment. “Could you give me a consult?” she asked. “Of Course”, I replied. We walked through the patient again, she had done everything right. They had started the patient on all the right medications, she had placed the patient on their belly. We reviewed the ventilator settings. It was clear there was really not much else I would offer the patient, even if we had the beds. With COVID-19, sometimes you can do everything right, and still lose the battle. I wished her good luck and asked her to call back if she needed me.
Part of my job of being an ICU physician is fielding calls from surrounding rural hospitals, and I’ve been getting alot of calls like this.
It’s not that my hospital is full of covid patients, quite the contrary, most of the patients in hospitals right now are the run of the mill usual patients. But on a slow day in winter time, a hospital is probably going to be at 60 to 70 percent capacity. COVID has changed this. Now most of our hospitals’ extra capacity has been taken up by COVID patients, leaving practically no room to take care of patients from small rural hospitals.
While small and often understaffed, rural hospitals serve an outsized role in managing illness in rural areas that have limited access to health care. Unlike large urban centers which usually have critical care physicians managing ICU patients 24/7, these rural ICUs are often managed by hospitalists or nurse practitioners. These smaller hospitals often don’t have the staff or expertise to take care of extremely ill patients that require specialized care. They rely on having the safety net of urban tertiary care centers to help manage those patients.
Only now, that safety net is being ripped away. Without it, I’m not sure how they’ll manage these tremendously sick and complicated patients. Without the ability to transfer to a tertiary center more patients will need to be treated in rural centers than otherwise would have, and certainly that raises the likelihood that more patients will die in those centers than otherwise might have. At this point, our only cure is prevention. I am pessimistic that we will convince people to take precautions that they have, up until now, seemed unwilling to take. It would seem, therefore, that the coming vaccine is our best chance to stop this before it spirals out of control. Having worked with small rural hospitals in the past, I know that they are filled with dedicated professionals, as good as anywhere else in the country. But there’s only so much that they can take. Only time will tell how these hospitals handle the surge that is currently ongoing but I fear what will happen if it gets worse.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, former CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
I’ve never been a gambler, so I don’t really know anything about the game of craps. I just see how it’s portrayed on the big screen–it always seems so fun and dramatic. A guy rolling the dice, surrounded by a group of cheering fans. He says something like “Seven, c’mon seven!” and tosses the dice in the air. For that moment, a drawn out moment, all the faces freeze in gleeful anticipation, watching the dice fly through the air, waiting with hope and anticipation to see where they land. It’s completely left to chance, or maybe luck, or perhaps prayer. For that moment everybody waits, everybody dreams. They live in that moment, waiting to celebrate.
The scene is very much like the one we find ourselves in now. The decision to reopen the economy has been made, the dice have been cast into the air, waiting to land. Already we’re seeing signs that the economy is improving, people are venturing out again for summer getaways. Restaurants and shops are reopening, and there are predictions of improvement in several economic metrics like jobs, and consumer spending. While we have metrics to measure progress on the economy, metrics that measure the concurrent COVID-19 risks are, unfortunately, terrible. In other words, while the potential winnings at the craps table are plain for all to see, the participants in this game are simultaneously blind to the downside risks. Like I said, I’m no gambler, but it would seem to me that a good gambler always knows their risks. Let’s have a look then, at the metrics we’re using to warn us of the risks in the gigantic game of chance.
COVID-19 Testing.
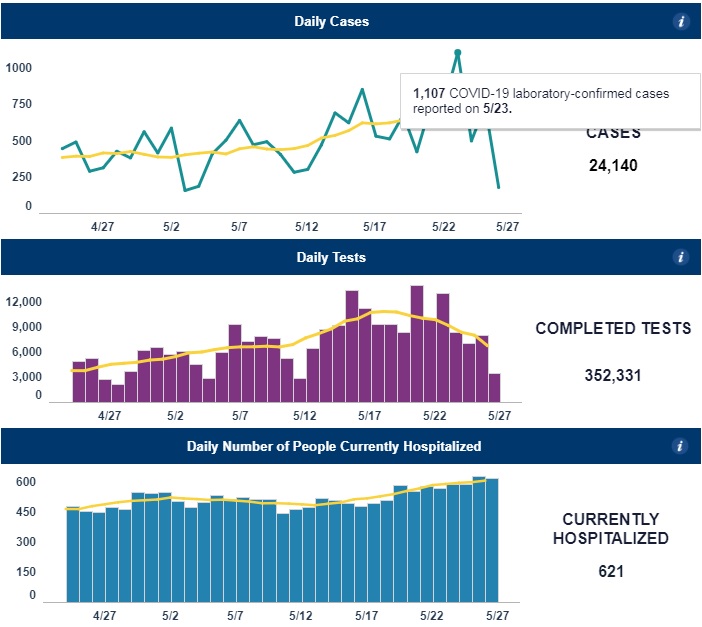
The media has never been very good with numbers, and the statistics heavy reporting during the pandemic has done nothing but reaffirm this. Media outlets continue to highlight “the new cases of coronavirus” without really putting them into the context of the increase in testing. Over this past Memorial Day weekend, media outlets reported that North Carolina experienced a record high number of new cases, with 1107 new cases reported on May 23rd. However they did not report the dramatic jump in testing that had also occurred. Looking at the graph below, you can see that testing has been increasing steadily over the previous weeks. Though if you look closely, you would rightly question my point, because on the day of the record spike, 5/23, there was a relative reduction in testing compared to previous days. This highlights another serious problem with testing, one that CDC director Dr. Robert Redfield recently eluded to when he said “testing sucks, bro”. Ok so he didn’t actually say that. But he did note that there are serious problems with data reporting, he stated that by the time the data reaches the CDC, “regularly the data is delayed and it’s incomplete.“
And for that, I hereby nominate him for the award of “Greatest Understatement of the Pandemic by Physician or Scientist”. To put it more simply, test result data is a freaking mess. The data on test results are reported by various different labs, at different times, and in different ways. Some of them might take a week to come back, some might take a few hours. While all labs report all of their positive results, not all labs report negative tests, or report them at the same time. Taking all of this together, if I were to look at that record number of new positive cases on 5/23 could I say with confidence that the data portray an accurate depiction of what was happening on that day? Not at all. The sad thing is that nobody really knows. We’ve taken to using moving averages of data not just because there is day-to-day variability in the data, but because there is a significant variability in the reporting of the data.
Percent positive tests.
The White House guidelines for “Opening Up America Again” called for a 2 week decline in the number of new cases to be achieved before proceeding to a phased reopening. However, it was apparent that as testing volume increased, case numbers would continue to climb. So as an alternative to this they also proposed that a 2 week decline in percent positive COVID-19 tests could also be used as a gating criteria. As with many things in life, this seemed like a good idea at the time, but later had us scratching our heads and wondering what we were thinking. COVID testing initially focused on high risk patients who presented to health care settings. As the pandemic has progressed and testing numbers have increased, we’re now testing more people who are not at the same high-risk profile. We’re performing more surveillance testing at group settings like nursing homes, prisons, and meat processing facilities. We’re screening people before surgeries and outpatient procedures. Screening these lower risk groups has the effect of reducing the percentage of positive tests. This in turn has the effect of making it seem like the prevalence of the disease is decreasing, when it may not be, and very likely going in the opposite direction. Now then, we find ourselves in a rather bizarre situation with two COVID-19 test-based metrics, total positive tests, and percent positive tests. Both of these metrics are telling us two different things yet both are somehow incorrect.
CLI: Syndromic Trending.
Every flu season, people start going to emergency departments and physicians’ offices with flu-like symptoms like fever and cough. Several of these locations are part of a statewide and nationwide network that track the seasonal flu. This system of patient care sites tracking symptoms of flu collectively make up the Influenza Like Illness Network, or ILINet. It’s a great system for tracking flu and gives clinicians a valuable tool as they make preparations for seasonal flu. Sometime in March, someone had the bright idea of using this network to help track COVID-19. It made a lot of sense, after all many of the symptoms were similar, cough and fever, and there was an obvious shortage of testing which perhaps this network could help make up for. At that time, it was the only way for officials to monitor COVID-19 activity. Thus ILINet was rebranded and the COVID-Like Illness Network, CLINet was born.
But there’s a number of reasons why this system, while great for tracking flu, is an imperfect tool for COVID-19 surveillance. First, the system requires that patients present to their doctors offices and ED’s with illness when they are sick. We know that around the country, patients are shunning visits to the health system, my own office visits are down about 50%. Even people with COVID-19 are delaying going to the hospital, and by the time they get there, they tend to be very sick. People are presenting to the hospital often a week or more after their first symptoms. This tells us that there is a considerable time lag between when people are infected and presenting to the ED. By the time CLINet tracks an upward trend, there will already have been a several week backlog of people who have been infected but haven’t yet presented to the healthcare system. In other words, CLI is what we call a lagging indicator, it’s not so much of an early warning indicator as it is an alert that screams “brace for impact!”.
Antibody testing.
Sars CoV2 antibody testing is emerging as an important way to tell if people have been exposed to COVID. It can’t really tell if there’s an uptick in infections, but knowing whether people have been infected is an important part of modeling. Knowing how many people have already been infected reduces the number of susceptible people, and thus the number who could potentially get sick from Covid. The antibody tests have a lot of positive things going for them, they’re relatively quick, painless, point of care, widely available and have fast turnaround times. As such, you’d think that they were the perfect test. Except there’s some issues with them. A positive test certainly could mean that you have had coronavirus, or it may also mean that you haven’t. Or maybe you’ve had another coronavirus that’s cross reacting with the test. With the current test we don’t truly know. But at least if you’ve had a negative test you can be sure that probably maybe have not had it. Or maybe you have. Again, it’s a tough call. For now, it appears that the antibody test will need to wait until the CDC determines that they’re no longer nearly useless.
Hospitalizations
Hospitalizations is probably the only indicator that we have that is not subject to errors from the various sources above. The obvious problem of course is that hospitalizations data is that they are a lagging indicator. If we wait until people start landing in the hospital, it’s probably too late to prevent more people from landing in the hospital. Aside from deaths, it’s the ultimate lagging indicator. Lagging indicators are not useless, they can help tell us when a surge has peaked and provide valuable data for modeling future outbreaks. But they’re not the indicator we need to help us determine when and where the next outbreak will happen and allow us to act in time to stop it.
What are the Metrics we Need?
Tests, tests, and more tests. In order for testing to be a more valuable metric, there needs to be many more of them. Testing sites need to be ubiquitous, and we shouldn’t have to wait 4 days for the results. Currently in the U.S we’re testing about 400,000 people per day, that’s much better than we were a few weeks ago. But several groups who look at the numbers of tests required to safely monitor the public are calling for much higher numbers, and there are a number of estimates that cover a very wide range. On the low end you have a group from Harvard calling for 900k tests per day at a minimum. At the high end there’s another group, also from Harvard, calling for 2 million tests per day to start, ramping up to 5 million tests per day by early June. Harvard apparently has a very large campus and it was too far for the two groups to walk and meet each other.
By increasing the numbers of tests in this way, we could more easily know the true prevalence in any given community, and see when it is increasing. In lieu of widespread COVID patient testing, we could be helped by some other metrics that give us clues about disease activity, and thus help in predicting disease outbreaks before they happen. Testing of wastewater samples, for example can identify the presence of coronavirus in a community even before the first case is identified. Kinsa, a smart thermometer, has shown that it’s aggregated data can predict disease activity 3 weeks in advance. Increased community mobility, as monitored by tech companies like Facebook and Google, can show that a community is at higher risk of a COVID outbreak. In fact IHME is now using mobility data in constructing their models of COVID activity.
Maybe we’ll finally get testing to where it needs to be. Maybe some of these other metrics will help in predicting future outbreaks before it’s too late to stop them. Maybe coming weeks will see more effective treatments for sick people and meaningful progress towards a vaccine. These are the only things that change the trajectory of the dice as they fly through the air. As healthcare workers all we can do is prepare, and wait for the dice to fall where they may.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
About a week ago, while getting ready to come in to work, I noticed my left eye was red. This gave me pause for two reasons. First because pink eye has become recognized as one of the many signs of COVID-19, and second because regularly perform bronchoscopy, an aerosolizing procedures on patients. I was referred by employee health to get a COVID-19 test. Except I couldn’t because while our hospital does offer it’s employees the option of drive-thru testing, that test is only available for limited blocks during the day, and that time had already passed. It was a Friday afternoon, now I would have to wait until Saturday to get tested. But on the weekends employee health does not offer the test at my hospital, so instead I would have to drive to a site 50 miles away from my house in order to get the test on Saturday. Instead of waiting, I opted to go to the outpatient testing center, the same place that I send patients to to get tested for COVID-19. After a quick drive-thru nose swab (take heart, it’s no longer the terrible brain tickler it used to be) I was on my way to self isolation at home until my results came back from LabCorp.
That process took 4 days. Fortunately they were negative, but let’s pretend that they had been positive. In the days since the bronchoscopy I had been interacting with people, co-workers and patients all over the hospital. Had I been infectious, I could have potentially infected many of them, after all we know that asymptomatic people with COVID-19 can still spread the disease. All of those people whom I had infected at home and work had continued to be out in the community for the 4 days since the time I took the test. Many of them may have gone to church (now open), restaurants (now open) and to their own homes. Each of these people would have to be tracked down and potentially tested, then those tests would take another 4 days. If the tests in those contacts had been positive, many of their contacts in turn would have to be tested, who would also have to wait another 4 days to get their test results. At this rate, my one infection could easily cause a breakout cluster that could not be contained. It would only be a matter of time before the disease would find a vulnerable person and kill them. It does not matter how many surveillance and tracking people we hire to track and isolate cases, if the tests take too long to come back, the disease will always be several steps ahead of us.
The President said that we have “prevailed” on testing. We have not, and still have much work to do. Testing was initially constrained by a number of factors, most recently a lack of reagents. As we have solved that problem we have run into a shortage of swabs, and now we’re again running short of PPE, in particular gowns. Testing is just one part of many interdependent parts that we need to get right in order to control the infection. Until we prevail on all of them we have not prevailed at all.
Everyone seems to want to talk about testing these days. The administration talked about testing when it, with much fanfare, rolled out it’s plan to reopen the country. “There’s plenty of testing”, they told us, we just needed to find it. They even did the leg work for us, providing governors around the country with the phone numbers of various labs that had unused capacity. Imagine that, we were scrambling to find more COVID-19 tests, when all over the country, lonely lab techs sat idling on their lab stools, staring at bunsen burners like modern day Maytag repairmen. The thing is, when they say capacity, it isn’t exactly the same things as ability. My high school guidance counsellor used to tell me all the time that I had the capacity to accomplish much more. And look how that turned out.
Yes, capacity exists, and I’ve written previously about how unused ventilators could be moved around the country when hospitals had a need. But ventilators and laboratories, I’m told by various somewhat intelligent people, are very different. Very very different. Labs for one, are made up of predominantly cinder blocks and have a tremendous number of people inside. Ventilators have no living things inside save for the 4 or 5 mice that make it run. Also they have wheels. So yes, there’s lots of capacity, but what good is that capacity if it’s on the other side of the state from me? The unused lab to which I send my COVID-19 test may take 2 to 3 days to provide a result. In the meantime, a patient is sitting in self quarantine at home, waiting for the results. That’s now 3 days of lost productivity, 3 days of worrying, 3 days of finding child care, multiplied by, oh I don’t know, let’s just say fifty thousand or so tests per day. When the country reopens, people need to be able to get tested quickly, efficiently, cheaply, and accurately. Right now I can’t that we even have one of those things.
Update on testing in my community.
In my last update I told you that things were looking up, as we had gotten Cepheid’s rapid test, which takes 45 minutes. It went well for about 10 days, but then our supplies of the test cartridges started to run low. Cepheid has not been able to keep up with demand, presumably they have prioritized hot spots to be supplied with more tests, and NC is not a hotspot. So while we’re still using this test for inpatients, we use a LabCorp test for ED patients not being admitted. On a bright note, the LabCorp COVID-19 test turnaround has come down to 2 days from its previous ludicrous time frame of 8 days. While that’s a positive development, it is still too slow.
Outpatient testing continues to remain beyond the horizon. We simply don’t have the PPE to spare for it. NC DHHS reports that as of today the state has a 1 day supply of N95 masks.
In the President’s most recent home shopping network episode on 4/27, he announced that testing would double in one month, home testing kits would become available, and reliable antibody tests would be available too. The President has the capacity to talk a whole lot and make a lot of promises, let’s see if they actually turn into action.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
Over these past few weeks we physicians have been thrown into the national spotlight literally risking our lives to care for incredibly sick patients under terrible conditions. We are heroes, at least for the moment, as well as victims of the COVID-19 epidemic that has washed over our country. Social media has become alight with all manner of healthcare workers posting themselves festooned in their protective gear, dancing, hugging, celebrating to the adoration of an appreciative public. I am writing this to appeal to you, to all of you. Please stop posting selfie pics and dancing videos of yourselves on social media**.
I get it, the siren song of the selfie image of yourself wrapped in protective gear, the portrayal of yourself as a selfless, courageous soldier answering the call to battle is too hard to ignore. Your social media posts bring you a form of hero worship that few people could ever hope to achieve. This is the validation that you’ve always known that you’ve deserved, and now it’s here, just like back in the Old Days. Doctors used to get a lot more respect back in the day, at least that’s what the older ones are always saying. Our profession used to inspire television shows, like, Scrubs, House, E.R, and that other one where they’re always hooking up. Oh, that one’s still on? Dear Lord, why?
But anyway, most of them are off the air now, and Silicon Valley is mostly trying to figure out how to replace you with self doctoring robots. Hell, your employers won’t even refer to you has “Doctors” anymore, you’re “Providers” now. I get it. Completely. Totally. Utterly. Get it. I know this because I am one of one of you. I too am a pulmonary, intensive care physician, and I too couldn’t resist the appeal of the self indulgent selfie. And yes, my posts also received the obligatory “your’re so brave, please be careful”-type of validation that I have never in my career experienced. But the fact remains. It’s time to stop.
These days every healthcare worker is posting selfies with themselves dressed up in their gear whether they’re on the front lines, or the back lines. Even cafeteria lines. You got nurses and the TikTok Doc dancing like they just scored a touchdown. I’m not sure if any of you folks are aware of this but maybe I should remind everyone. Nearly all of your vented COVID-19 patients died. 50,000 of them by my last count, probably a few thousand more by the time you’re reading this. We in health care have pretty much had our asses handed to us, so I really can’t figure out what y’all are celebrating. You should be as somber as a team that just got destroyed in the SuperBowl. Not only are we losing, when people are coming to us, we got nothing for them. We have no treatments, no proven medications, no procedures. The only advice we can give people is to avoid getting it, and that by literally eliminating any possibility of contact with all other human beings. This is why you must stop. Please.
It’s gotten so bad that the President. . . The President of the United States. . . is now the nation’s greatest authority on “chloro, uh, hydroxy” something or other.. And yet, somehow, inexplicably, despite the deaths of more than 50,000 souls under our care, WE have been cast not only as heroes but also the victims of this tragedy. And so here it is, if you haven’t figured it out already. This is THE REASON why you have to stop.
Symbols are powerful, they’re totems marking the passage of sentinel events in our history. People connect with them, and they help to humanize events, allowing us to empathize with the people involved in them. After 9/11 there was the imagery of the twin towers crashing. After Katrina there were the images of people stranded on roof tops. Both events spurred the American public to action with record levels of donations and volunteerism. What are those same Americans doing in the face of this tragedy? They’re making masks for healthcare workers, they’re donating money to buy PPE. Around the country church groups are organizing, girl scouts are canvassing, companies are volunteering machinery and equipment. . . to make you a new frigging face shield. Go right now to any of your social media feeds. What volunteer work and fundraising do you see? Have you seen anyone trying to raise money for the more than fifty-thousand victims families? No. People are mostly just trying to raise money in support of healthcare workers. And that my friends, that’s why you need to stop. You have unwittingly taken on the victim role, instead of the true victims.
There’s another tragic consequence to the role that we’ve taken on. People right now are protesting their stay-at-home orders. This pandemic’s lack of symbols has hurt not only fundraising for victims, it’s leading to people taking unnecessary risks. This has been an invisible tragedy, a silent pandemic whose deaths occur in locked ICU wards where families can’t be with loved ones when they die. Tens of thousands of people have left their loved ones to enter an ED or ambulance, only to never be seen by them again. Some can’t even have a proper funeral. People can not fear what they can not see, nor can they empathize with numbers on a screen. In place of the real victims, healthcare workers have become stand-ins, usurping America’s sympathies. And her dollars. That’s another reason that you need to stop.
It’s not your fault, the media bestowed this mantle upon you. You took it to show people how dangerous your working conditions are. You were right to do that, it really should not have gone further than that. Yet it did. But it’s now time for us to return to our primary responsibility, taking care of people. If we can’t cure them when they come in, the least that we can do is shine a light on this tragedy to maybe prevent them from getting sick in the first place, while also honoring the real victims. We have to make people out there understand what the true nature of this disease is. We must bring life to the cold numbers that people are seeing on their television screens, and to do that we need to speak for the victims and their families.
So stop posting about yourself. Post instead about the victims of this tragedy, the real victims. The poor patients who came to us. The poor people who struggled and died. The poor people who pinned all their hopes on the chance that we might be able to save them. We couldn’t, we didn’t and now we should honor them by telling their stories.
I hope that in this way we can move the media’s focus from us to the real victims of this tragedy, and get them the coverage, support, and empathy that they deserve.
**Unless you’re a NYC healthcare worker. You’re a hero so please post whatever you want.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
Right now pulmonary critical care physicians are fielding myriad calls and texts from all over the country. These callers come with frantic questions. Questions like “Hello Deep this is Minnie, your aunty. Your uncle’s toe is hurting and I read on the internet that it’s a sign of coronavirus. What should we do?” Notice that they don’t ask “could I have coronavirus?” because they are absolutely convinced that they have it. What they want to know is “what should I do about my coronavirus”. Of course I give them the usual measured, sober and socially acceptable response; You’re ok, stay at home, wash your hands.
But here’s what I WANT to tell them.
You beat coronavirus? Celebrate, CELEBRATE, YOU’RE FREE! Throw away your hand sanitizer! Run to the grocery store and grab an unsanitized cart, feel free to touch every cereal box. Use the bathroom and dry your hands with the air dryer. Take in a movie, get some popcorn, and go ahead and lick those buttery fingers. No need to be afraid.
Soon, we’ll be through the initial hellish phase of this pandemic with it’s spiraling death counts. But the fight won’t be over. Until we have an effective vaccine or treatment, we’ll enter a prolonged stalemate with the disease. Now that we’re looking at opening the country back up again, people have been contemplating what that might look like.
That future will inevitably split us into two groups based on whether we have immunity from the disease or not. Immune people will have their status bestowed on them from previous infection or documented by results of antibody testing. Eventually someone will come up with a catchy title for Immunes and Uninfecteds. Perhaps there will be a Twilight-esque movie about a forbidden romance between the two. Spoiler alert, one of them dies.
Life for Immunes is going to be good, their lives will look, to the Uninfected, like an unending party. They are going to go out early, and stay out late.They will restart their lives, and live them like it was the last day of their lives, such will be their appreciation for their rewon freedom. Uninfecteds will still be staying at home, watching the glamorous lives of the the Immunes as if from behind prison bars. While people will know their own status there will be no way to tell who is who in public. For that reason, governments will still require some form of social distancing to protect these people. Many Uninfecteds will with violate that, and they will get sick and die.
Immunes will feel sorry for the Uninfecteds, “I feel really bad for Uni’s” they will say, “but I have to work and feed my family. Why should I go on with the quarantine when I’m not sick and there’s nothing wrong with me?” Life for Uninfected’s will be tough. They will eventually need to go back into the workforce. But in order to work they will need to have protections against infection.So they’ll ask for accomodations from their employers based on the American with Disabilities Act. And as they are accomodated, workplaces will become increasingly segregated as Uninfecteds seek protections like individual spaces with appropriate physical distancing. They’ll have different restrooms, different lines in the cafeteria and different dining tables. In some cases an Uninfected worker will be paired with an Immune for their own protection. The Immunes will naturally resent the social isolation. The Uninfecteds will see the Immunes new found freedoms and resent them right back.
Meanwhile the employment pictures will look very good for Immunes, particularly health care workers. While employers will insist that they do not discriminate based on immune status, everyone knows that they do. Employers know that Uninfecteds could get sick and then require time off that could range from a few weeks to a few months. Even worse, they might die. For that reason, insurance premiums, including life, disability, and health insurance, rise astronomically for Uninfecteds. For all of these reasons Uninfecteds have a much harder time finding work especially obese men over 50 who appear to be more affected by the virus.
After the tragedy of the intial part of the health crisis in the U.S., healthcare workers were seen as heroes and had enjoyed a new found solidarity. That quickly falls apart as health care systems bid up the prices on Immune workers. Across the country every one is tested for antibody status, laws are passed requiring that everyone have their COVID-19 Antibody status determined.
Health disparities that existed before the crisis become wider, while new disparities emerge. Covid-19 antibody status becomes a ticket to a better life. Illicit dealers emerge to sell samples of the virus to people who want to infect themselves. Political differences emerge too, one political party declares itself a champion of Immune freedoms. SImultaneously they accuse the other party of promoting a socialist agenda by promoting accomodations for Unifected.
The Immune party blocks a bill in the House stating that it is an invasion of privacy, but it’s really about blocking funding needed to build factories to make the vaccine. The vaccine is now the only thing that separates the Immune from Uninfected. Facebook posts appear showing the dangers of vaccination, stating that the vaccine come from a WHO plant built by the Chinese. The vaccine, it is rumored, contains another secret virus. This virus, they say, is even deadlier than COVID-19. And the new virus would do things to our country that no one could imagine.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
In my last post about the status of testing for Covid-19 testing, things were not going well here in North Carolina. Our inpatient testing time was up to 8 days through LabCorp, and we had completely stopped any outpatient testing, including drive-through testing.
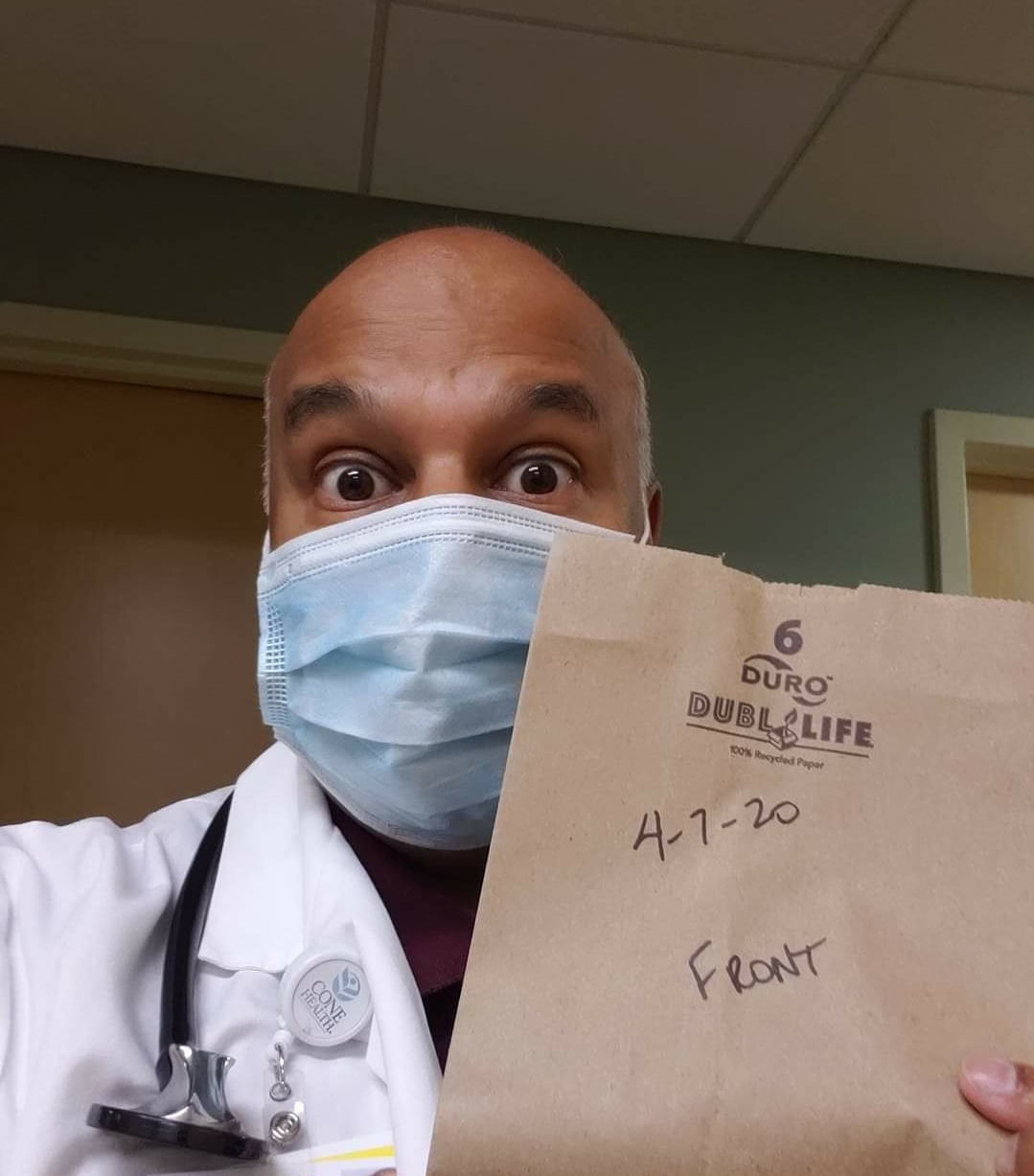
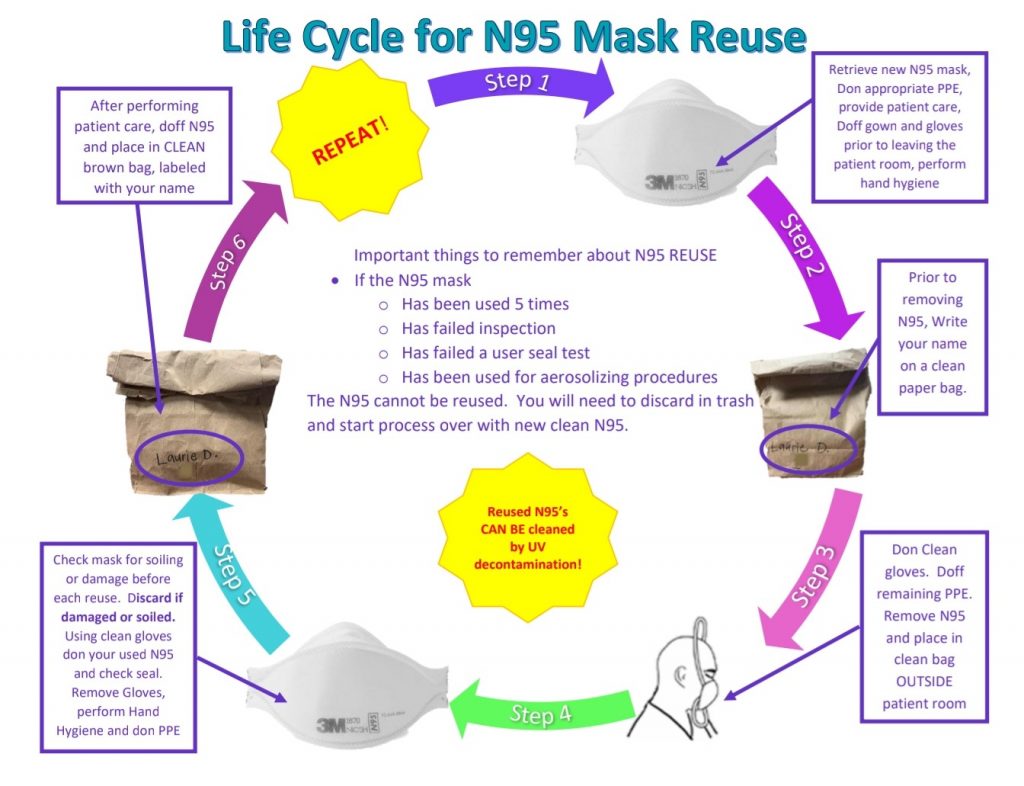
PPE supplies remain short for our health system, particularly N95 masks, and our hospital has been working tirelessly to acquire more but most of our orders have gone unfilled or partially filled. To that end we have adopted CDC guidelines on how to recycle the disposable masks to prevent us from running out completely. As you can see from the figure above, the system upon which our lives and our patients’ lives depend, hinges on the use of brown paper bags. This is not exactly the high technology we imagine when we think of American healthcare, yet that is where we are at now.
This is how the process works; when leaving a COVID-19 patient room, we write our name on a brown paper bag as well as the number of times the mask has been used, then drop the mask in the bag and leave it at the entrance to the patient’s room. That mask is then only to be used by that healthcare worker with that patient. Each time they use it, we update the number of times the mask has been used. Once the mask has been used 5 times, the mask is discarded. We have supplemented this by using U.V. light to disinfect the masks between uses to help reduce the chance of spread.
In the meantime I am glad to report that at least our local testing situation has improved. Up until this week we were having to wait an excruciatingly long 8 days for inpatient COVID-19 test results (we’ve already given up on any semblance of outpatient testing). By contracting with a lab in Texas, we have gotten the test results down to 2 days. Sometimes it’s one day, and that literally depends on (believe it or not) if the sample can catch the 8 pm out of RDU.
Abbott released a 15 minute test on their IDNow platform. I discussed previously why that is not an option for us, and indeed not an option for many at all. Our hospital uses the Cepheid’s GeneXpert system and they’ve come out with a test with a 45 minute turnaround time. Like Abbott they, too, have been focusing on supplying new test cartridges to hotspot areas, which fortunately we are not. Hopefully once these surges have calmed down we might have access to that test and, at long last, be able to actually start screening people outside of the hospital.
Meanwhile, I’ll continue to soldier on with the testing and PPE that we have and do the best I can.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
The loss of life from COVID-19 in the U.S. has been astonishing. The Surgeon General described this as our 9/11 moment. Yet most of us who are old enough to remember 9/11 can tell you, with vivid detail, what we were doing during the 9/11 attack. Yet I can’t say that I remember where I was or what I was doing when the death toll in our country from COVID-19 passed twenty-thousand. Can you?
2. Not a Made-for-Television Tragedy.
Unlike past national tragedies in the modern media age, there is no national symbol for COVID-19. There are no images of burning buildings like in 9/11, no images of people stranded on rooftops like after Katrina. The deaths and suffering from this disease are largely ocurring behind closed I.C.U. doors. Families are often times not allowed to be with their loved ones as they die due to infection concerns. Families and friends are being denied access to funerals and are forced to grieve alone. Yet there is no national symbol to cyrstalize this tragedy. We need a moment around which to rally, commemorate, and grieve.
3. We need to raise money for families.
Flowers are left outside refrigerated trucks used as makeshift morgues at Wyckoff Heights Medical Center in Brooklyn. Credit…Sarah Blesener for The New York Times
American’s empied their hearts and their wallets for victims of previous tragedies. After 9/11 a record $2.8 billion was raised in donations for victims’ families. That record was broken after Hurricane Katrina which saw $5.3 billion in donations to victims. For families, the loss of loved ones could not have come at a worse time, just as the country tips into recession and millions of people have lost their jobs. They will need help, and we should be there for them.
4. Healthcare workers need a moment.
skaman306 / Getty Images
While the fear, misery, and heartache of this pandemic have been barricaded inside locked hospital wards, it does not remain there. It is carried out on the shoulders of the healthcare workers who stream in and out out of them. Often times they are working under harsh and dangerous conditions, worried about infecting their own families. Yet despite these conditions, they are under threat for raising issues of workplace shortages. Healthcare workers need a minute, just a minute, to look over our shoulder at the turmoil behind us. Then we can start moving again.
Despite the tremendous loss of life, there has been precious little talk of victims, save for the occasional mention of a celebrity death. The media has instead focused on political aspects of the pandemic, assigning blame for shortcomings in testing and treatment. In the meantime trenches are being dug in New York to bury unclaimed bodies. The media needs to stop the political drama and help us learn about who these people were. Their bodies may be unclaimed, but their stories should claimed by all of us. No one should die faceless and nameless in America because this is not that kind of country and we are not that kind of people.
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
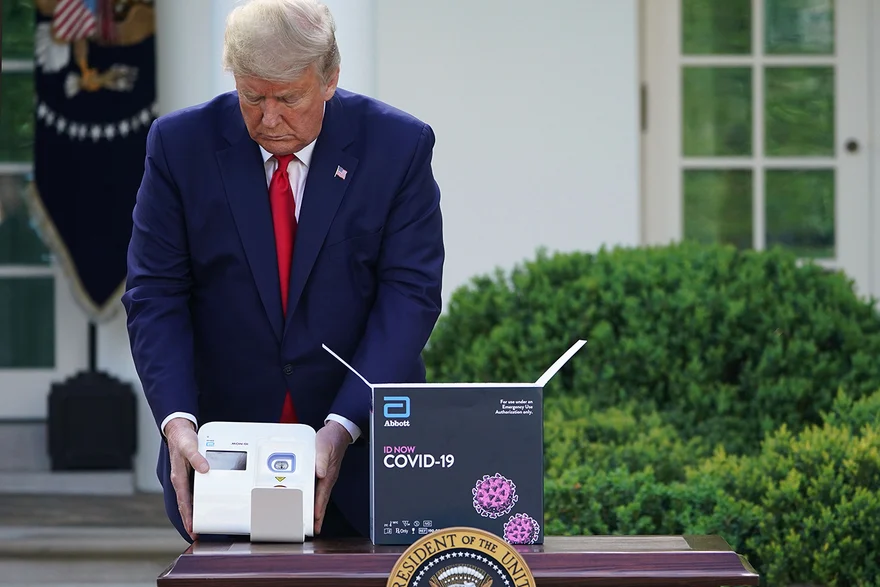
Is it me or are presidential press conferences turning into infomercials? There is a reason that the federal government doesn’t want physicians accepting gifts from pharma. There is a reason that we all thought that direct to consumer advertising is a bad idea. When medical company reps speak with physicians, they are tightly bound by laws that limit them from making false claims about a product. A physician with bad information can not only harm people, but they can waste lots of money in the process. It would probably make good sense to have similar restrictions in place when a CEO speaks with leaders in DC who hold sway over billions of dollars. But then we wouldn’t be able to have the direct to consumer advertising that is President Trump’s daily COVID-19 updates. It’s no secret that any company would love business right now, but know what else they’d love? How about free advertising with a side of ‘Murica.
What better place to do that than a nationally televised Presidential press conference with incredible ratings in the middle of a crisis, where no one literally has anything to do except watch television? I mean if you can’t expect a physician to critically appraise a new medical product in the face of free salami, you can hardly blame the President for going gaga when Abbott told him they would save his beautiful, amazing, beloved, best-ever in history economy by pushing out half a million tests.
One can only imagine the President’s excitement when Abbott Labs informed him that they planned to produce 50,000 tests per day. Also they gave him one of his very own to play with. My contacts in the West Wing tell me that not only is he testing anybody who comes to visit him, he also tests Mike Pence several times per day just so he can see the lights change color.
But there may be a few details that Abbott’s CEO kept close to the chest, such as the fact that just because you make half a million tests, this does not translate to half a million real life people being tested.
To put it in terms the President might relate to, they would have to explain it like this. Making a COVID-19 test is like making an Atari game. Even if I give you half a million Atari games, you can’t play any of them unless you also have an Atari console. A few hospitals out there have Atari consoles and will be able to run these tests. (Yes I realize I’m mixing metaphors but just stay with me). As for the rest of the hospitals, well I’m sure that Abbott would be just super excited to sell them one at some point in the future. Right now though Abbott only has a few, and they’re going to a few designated hot spots. But if you know nothing else, just remember that Abbott is making the rapid COVID-19 tests, no one else is, you can buy one eventually, and if you feel at all nervous about this plan please relax and listen to this soothing recording of Michael Bolton’s greatest hits.
So really, what Abbott sold the administration is an imaginary number based on the potential tests they could make, not necessarily the actual number of tests that would be run. In their press conference on 4/8/20, Dr. Birx admitted as much, stating that the number of tests run are nowhere near the numbers that Abbott suggested. But more than selling the President on a plan, what they really sold was alot of future ID Now consoles. And in the end, isn’t that what’s most important?
Deep Ramachandran, M.D. is a Pulmonary, Critical Care, Sleep Medicine physician, founding CHEST Journal Social Media Editor, and co-Chair of ACCP Social Media Work Group. He blogs at Caduceusblog. He is on twitter @Caduceusblogger.
My office practice has been slow here in North Carolina. I have been doing all of my patient visits via telephone, but even those are becoming rare. So I was glad when I got a call to see a patient with respiratory problems up on the wards. The patient herself was an elderly woman with an abnormal CT scan who had also undergone a test for Covid-19. Those tests are taking 8 days or more to come back unfortunately. Like many patients we test, it’s like that she would be discharged home before getting the results. Her doctor asked me to see her to see if the pneumonia they thought she had could be Covid-19. Looking at her CT scan I knew coronavirus was not the main problem, she had a lung mass which was probably lung cancer.
In order to minimize our exposure time to infected patients many docs have been in the habit of calling in to the patient’s room to speak with the patient before entering the room for an exam. Impersonal yes, but probably safer. So picked up the phone and dialed into the room. As I pressed the phone against my ear I immediately regretted the decision. Thinking through the countless e-mails and meetings about Covid-19 preparation, I couldn’t think of one that mentioned anything about a phone sanitizer guy. Luckily I was bailed out by a busy signal.
So I got up and walked over to the PPE station. This would be my first experience with PPE. Unlike NYC, New Orleans, and Detroit, Covid-19 is still new at relatively new at hospitals in North Carolina.
I had sat through a PPE demonstrations a few weeks ago, there weren’t enough PPE for each of us to try it ourselves but I was pretty sure I got the jist of it. The process started with choosing a face shield or goggles. Apparently I’m a goggle guy. The patient was under droplet precautions, not airborne, which meant that the infamous N95 was not required, so I donned a surgical mask. Then it was the blue plastic barrier, finally gloves, and into the room I went.
I’m always amazed at the resilience and courage of so many people when they hear that they have cancer. I do the best I can to be in the moment with them, there’s tears, touching, hugging, prolonged silence, questions, and more tears. It must be especially hard being told of this in such an impersonal matter. Our words competed with the loud device that recycled the air. As I hugged her I was somewhat self conscious about how it must feel through the cold shiny plastic that I wore. There was no way for her to see any of my expressions, my smile, my magnificent smile that everyone always compliments me about. I usually offer to call family for patients to help explain the diagnosis to them in the presence of the patient. I offered the same to her, but then I realized that taking out my phone would violate precautions, so the call would have to wait.
I left the room, and was immediately met by a spotter who guided me through the doffing process. As I went through the steps I started thinking about what had just transpired. Covid-19 has just arrived and will be with us for at least several more months, if not longer. Lung cancer, too, is not going anywhere. I need to get better at this.





 Look at this idiot.
Look at this idiot.
:strip_exif(true):strip_icc(true):no_upscale(true):quality(65)/arc-anglerfish-arc2-prod-gmg.s3.amazonaws.com/public/DF65YKARRNGKLGTOXGO27JG43M.jpg)