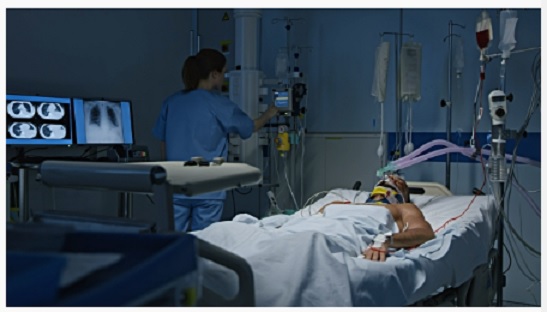
May lay in a hospital bed, her wrinkled and mottled skin covered with leads, and sensors that monitored her every breath and heartbeat. A camera that was mounted on the wall allowed a doctor to zoom in closely enough to count her tattered eyelashes. Her husband sat at her bedside, gently stroking her withering gray hair as her chest moved slowly up and down accompanied by the soft whoosh-whoosh of the ventilator that breathed for her. He stared expectantly at her face as if at any moment she would rise and free herself from the myriad tubes that sustained her. Her adult daughters sat and stared blankly at the floor, waiting for something, anything. The streams of data transmitted from her body were monitored closely both by a team in a remote electronic-ICU bunker 50 miles away and her ICU nurse 15 feet away. Yet what May could not have realized was that despite her family’s presence at her bedside and the twenty-four hour care she received, she had been abandoned. She was alone.
Several weeks earlier, May came to the hospital from her nursing home, “yet another pneumonia”, the note in her chart said. “She seems to get one of these every few months” said her husband “can’t we give her something for that?”. The Emergency Room physician explained that she had aspiration, essentially choking on her own food and spit. She would continue to get pneumonia, until she eventually passed away. This wasn’t the first time he had heard this. “They told me before to let her die, but I didn’t listen to them, I told them to treat her anyway, and she made it through. I didn’t give up on her then and I’m not going to now”, adding “she’s a fighter”. Her husband Daniels countenance was such that the Emergency physician admitting May to the hospital didn’t bother asking whether his wife should be resuscitated in the event her heart or lungs stopped working and she needed to be put on life support. May was admitted to the general medical ward, and was started on antibiotics, but she eventually got worse. Sometime in the middle of the night a nurse found her ashen and struggling to breathe, and called a “code blue”. May’s breathing had gotten so bad that she needed life support, she had a tube put down her trachea and was taken to the ICU where she was put on a ventilator.
Doctors worked on her for more than a week, treating her pneumonia with powerful antibiotics. But even as her pneumonia cleared, her body withered. Her skin hung from her bones as her muscles wasted away, her eyes hollowed, and the skin of her arms filled with bruises as nurses struggled to find a place from which to draw blood. On the second Sunday of her ICU stay, the doctors tried a “trial extubation”. As the family understood it, her lungs had improved to the point that she might be able to be taken off the ventilator, but her body was now so weak, they did not know whether she would actually be able to breathe on her own. If she had to be put back on the ventilator, the doctors told them, she would require a tracheostomy that would allow her to live on the ventilator long term. The social worker would then seek placement in a long term facility for patients on long term ventilators, essentially a hybrid hospital, rehab, and nursing home in one. Her breathing failed within minutes of being taken off the ventilator, and she was immediately put back on life support.
It was the following day, Monday morning, that I met with May’s family to discuss what had happened the day before, it was the beginning of my ICU week. For May and her family it was the beginning of their third week in the ICU, and it showed. Her husband, Daniel looked unkept, his thick shock of gray hair was whirled and tangled, his flannel shirt partly tucked into ripped and stained jeans. He gave the impression of someone who had not been taking care of himself, let alone someone who could take care of his chronically ill wife. His visage upon seeing me betrayed both surprise and regret as he recognized me from four months earlier. I was the doctor who told him that May was going to die. Continue reading “Not Dead but Not Alive; The terminally unhealed languish in America’s hospitals.”